
Pregnancy is a stage of hope and joy, but also of fears and uncertainties in the face of a situation that, being natural, is at the same time extraordinary. Childbirth is often as desired as it is feared. One of the things that worries future moms the most, apart from the pain, is if the baby will be well seated in the pelvis and if your posture will be adequate to come out easily in a vaginal delivery.
In general, the baby is placed in the "exit position", more or less from the eighth month of gestation, but this can happen later or even shortly before delivery if the woman has already had children. This is known as nesting. The baby is descending and placing itself in the mother's pelvis, usually with the head down, but can sometimes adopt other postures.
The position of the baby in the uterus can be known through ultrasound scans. Experienced midwives can also know the position of the baby by feeling the mother's belly. However, until At the moment of delivery, it is not possible to know with certainty the position the baby will adopt to go out since, although in the last weeks the space is reduced, the amniotic fluid allows some mobility. In addition, sometimes the same labor contractions cause babies who come in one position to change at the last minute.
Knowing the presentation in which the baby is in the last trimester is very important since it largely determines the development of labor. In 1996, New Zealand midwife Jean Sutton published, together with prenatal teacher Pauline Scott, her book "Understanding and teaching the optimal foetal positioning" (understanding and teaching the optimal fetal position). In it, they develop the theory that the movement and postural changes of the mother in the last weeks of pregnancy can influence the posture that the baby adopts at birth. This is of vital importance since, according to this theory, many of the difficulties at the time of delivery are due to the fact that the baby's presentation is not optimal for it to develop normally. But what is the optimal fetal position and what can we do to achieve it?
There are three types of presentations of the baby in the womb: cephalic (with head down), breech (breech) and transverse (The baby's head is on one side of the mother's womb and its rear is on the opposite side, forming a 90º angle with the axis of the uterus).
Cephalic presentation
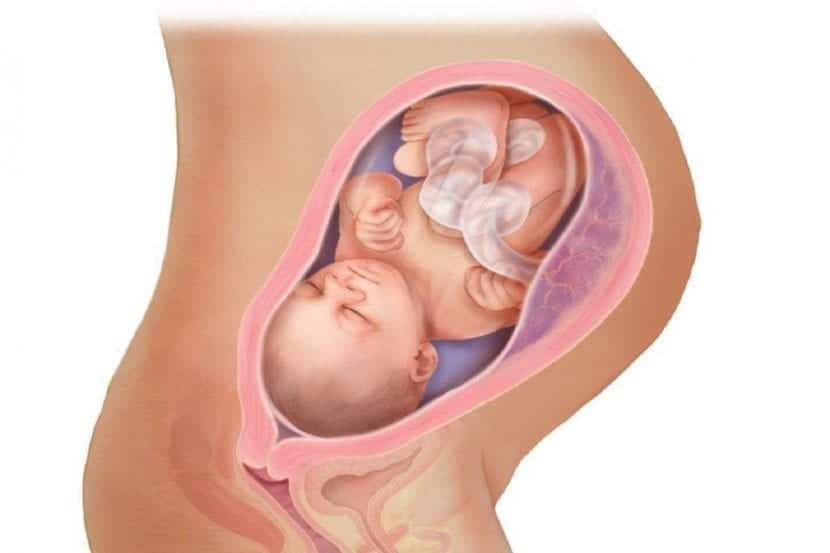
Most babies are in the cephalic position at the time of delivery, that is, with head down and buttocks up. Within this presentation there are two types: anterior cephalic and posterior cephalic.
Anterior cephalic presentation
The baby is upside down with his back close to the mother's belly. This would be the pideal position for birth. The baby's head flexes, with the chin resting against the chest and the crown (narrowest area of the head) being the first to cross the birth canal.
Posterior cephalic presentation
In this presentation, the baby is also head down but with his back close to the mother's and his face facing the belly. In this way, the baby's head is not flexed, nor its chin tilted, so your posture is less flexible in adapting to the birth canal leading to longer and more painful labor. This position does not imply that a cesarean section has to be performed, the delivery may be vaginal but it is likely to take longer because the baby's descent is more complicated.
Breech or breech presentation
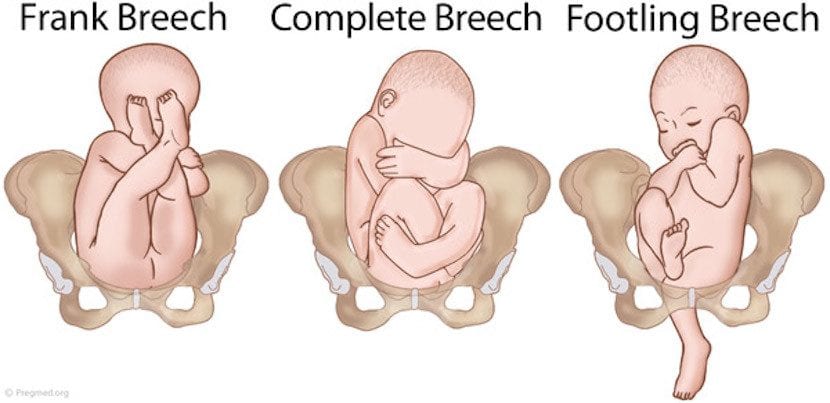
In this position the baby's head is up and the buttocks are down. That is the baby's pelvis is in contact with the mother's pelvis. Normally the baby is placed in a cephalic position between weeks 28 and 32, but others roll over several times before delivery, especially if there is excess amniotic fluid. Some, approximately 3%, never turn around and remain in a breech or breech position.
The fact that the baby is in the breech position in the last weeks of pregnancy often generates anxiety in future mothers since the breech baby is usually associated with cesarean delivery. But, is a cesarean section really indicated in these cases? Can a vaginal delivery be attempted?
In 2000, the results of a large study called "Term Breech Trial". According to this study, in breech presentations, cesarean section should be the method of choice over vaginal delivery since it seemed to decrease neonatal morbidity. These results were quickly accepted by the international medical community who chose to schedule caesarean sections rather than attempt vaginal deliveries when full-term babies were presented in the breech position.
Although the recommendation of the Term Breech Trial was adopted by most of the important international organizations in the field of health, among them the SEGO (Spanish Society of Gynecology and Obstetrics), there were some, such as the Directorate of Health Assistance of the Ministry of Health of the Basque Government, which decided not following these recommendations based on the fact that their health contexts, protocols and professional skills were different from those of the countries that had participated in the study. For this reason, successful vaginal deliveries continue to be performed in settings where there are experienced health personnel.
After this study was published, numerous articles that questioned its validity since in all the analyzed deliveries the recommendations for assistance to breech deliveries had not been followed. According to these recommendations, the interventions had to be minimal and all deliveries had taken place in highly medicalized settings. In 2006 another study was conducted, four times larger than the Term Breech Trial. In this study, called PREFASHION, it was seen that there were no significant differences in neonatal and perinatal morbidity between vaginal breech deliveries and caesarean sections. Currently, the SEGO, no longer recommends cesarean section as the first option when the baby is breech Rather, it leaves the door open to a vaginal delivery as long as certain conditions are met: correct fetal development and weight less than 4 kilos, that the baby does not look up and that it is positioned with the buttocks or feet embedded in the canal of Birth.
Transverse Presentation

In this position, the long axis of the fetus forms a 90º angle with the axis of the uterus, that is, its head is on one side of the mother's belly and the buttocks on the opposite side.
In this case, contrary to the breech presentation, it is dangerous to attempt a vaginal delivery since there is a high risk of injury and even death for both the baby and the mother.
What can you do to get your baby into the optimal position?
As we have already seen, the ideal for delivery is for the baby to be placed in the anterior cephalic position. However, if your baby is presented in other positions, do not be overwhelmed since in the last weeks or even during delivery there is a possibility that he will turn. Some Tricks and techniques can help your baby stay or get into a cephalad position.
Pay special attention to your posture
The postures in which your belly is lower than your back favor the baby to be placed in the anterior cephalad since, due to the effect of gravity, the baby's back will tend to be placed in the lower part of your abdomen. Try to tilt your pelvis back when you are sitting, ensuring that your knees are lower than your hips and avoid postures in which you are reclining backwards since your back is lower than your tummy favoring your baby to be placed on the posterior cephalic.
Practice exercises that promote optimal fetal position
Swimming is an ideal exercise for your baby to get into a cephalic position. The best is that swim upside down and avoid swimming on your back to favor the correct positioning of the baby.
Practice yoga for 10-15 minutes a day, especially the posture of the cat and that of the Mohammedan. The cat pose is performed on all fours with the hands aligned with the shoulders and the knees separated at the hips. The back is arched upward with the chin down, and then slowly stretches until it is straight as the head is raised. The Mohammedan posture is carried out by standing on all fours, bringing the trunk back and pressing the chest to the ground with the arms extended forward.
Use one Pilates ball for rocking exercises especially those where you lean forward.
Take advantage while watching TV to sit in a chair facing the back and leaning on him astride. You can also kneel on the floor leaning on the chair or on cushions.
External cephalic version

The external cephalic version is a set of maneuvers, which are performed on the mother's abdomen, to get breech or transverse babies into the cephalic position. Before carrying it out, an ultrasound is performed to determine the exact position of the baby, the fetal heartbeat is monitored and a medication is applied to relax the uterine muscles and make the process easier. Then the gynecologist will proceed to press on different points and perform gentle massages to try to position the baby cephalad.
The external cephalic version is a quite safe technique and with a high success rate, but it has the disadvantage that it can induce labor, so it should only be carried out in a medical setting and with full-term babies.
Moxibustion
This technique is recommended by the WHO for the breech presentation of the baby and can be performed from week 32 on. It is a technique of traditional Chinese medicine that consists of stimulate different points of the body with the heat of the combustion of mugwort (Moxa), an herb that appears to stimulate pelvic and uterine blood circulation, as well as adrenocortical stimulation that ends up stimulating fetal activity. In the case of breech presentation of the baby, point a stimulate is the outer area of the nail of the little toe. The success rate is quite high as shown by various studies, and unlike the external cephalic version, it does not have the disadvantage of being able to induce labor.
As you can see, until the last moment there is a possibility that your baby will turn around and you have different resources at your fingertips to help him. In principle there is no need to schedule a cesarean section. In addition, this also presents risks as it is a surgery, so the benefit-risk ratio must be assessed. In any case, if it is essential to do it, you should know that it is not necessary to schedule it since it can be done once the delivery has started. This way your baby benefits from the previous labor that will help him to adapt to the extrauterine environment. If your baby is breech or transverse, first of all keep calm as all is not lost. And above all, whatever your position, try to enjoy the unique and unrepeatable moments that pregnancy offers you.